Submitted to Keele’s Director of HR and TU Oversight Committee, 16 July 2020. Any responses to questions will be published when we receive them.
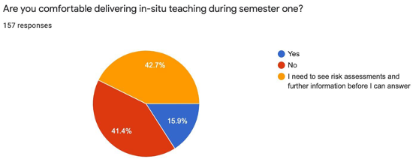
In order for Keele UCU to undertake its representative and statutory duties, we conducted a one question poll of members which produced the following result:
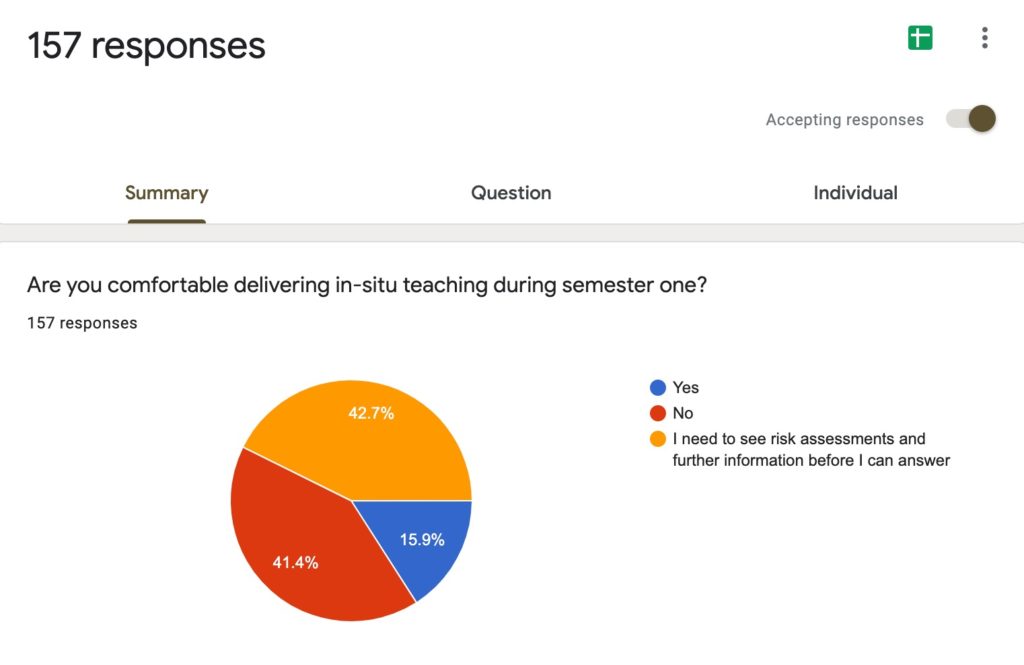
(Sent to members 17:00 10 July 2020. Results up to date as of 09:45 on 16 July 2020)
To understand the complexities of staff concerns about safety, we also asked for comments. From these, we have produced the following set of points which we ask those charged with risk assessment and risk management to consider. These are preliminary questions and further ones are likely to be generated as Keele UCU receives more comments from our members.
- There is widespread recognition that for most staff, students are the most significant hazard. What is being done to ensure that this hazard, not just the physical environment, is controlled and staff are protected from what students may bring into a classroom and other shared space?
- Notes that infection rates amongst 20-29 year olds are increasing at the fastest rate
- Notes that significant number of 20-29 year olds are asymptomatic, significant number have mild symptoms that may present as a cold or allergies
- Notes that students are expecting a return to social life on and off campus, and that effective physical distancing should not be assumed (evidence emerging on impact of this amongst 20-29 year old age bracket)
- Notes that risk of serious disease increases at a significant rate starting at age 40, and that most staff on campus are above the age of 40.
- What will the messaging be for students to remind them that ‘just a cold’ might not be just a cold? Students don’t have the best track record of not going to class when ill, and many of us can tell stories about students coming into our offices to tell us they have the flu and won’t be in their tutorial.
- What are the arrangements for on-campus isolation of students with symptoms/exposure/positive test results?
- How will students access testing? Esp. for students without cars. Postal test means breaking self-isolation to collect, so what will process be?
- What will the testing regime be following confirmed cases on campus/of students, staff or visitors to campus?
- Who will be responsible for the care and welfare of any students who experience significant (debilitating) illness within student accommodation? (medicine, food, home based medical care, welfare checks, etc).
- What are plans for contact tracing/test, trace, isolate? Are we depending on government provision, or are we developing something more effective?
- How will this take place?
- Who will run it?
- How to factor in student accommodation/social spaces? Public transportation? (45 minutes by bus from station to campus)
- Given it is likely that airborne, aerosol transmission is a primary source of infection (and that there is no documentation of infection through fomite transmission), the university must do more than tell us to wash our hands and provide hand sanitiser. Are the measures they’re putting in place demonstrating that they understand the scientific evidence informing changing knowledge of what the risks are? If not, can they speak with staff members who can help them with this?
- What is being done to ensure sufficient levels of fresh air ventilation in all rooms where teaching, face-to-face contact, corridors, and gatherings of more than 1 take place? Given the amount of evidence confirming high risk with indoor activity in closed space, this is vital even with 2m distancing being in place
- (please refer to guidance produced by US NiH, US CDC, University of Minnesota Center for Infection Disease Research and Policy on rates of sufficient ventilation; see, for a start, Kumar and Morawska, City and Environment Interactions, 2019; Li, et al, ‘Evidence for probable aerosol transmission of SARS-Co-V-2 in a poorly ventilated restaurant’, 2020. For lay science, there are some very good recent articles in The Conversation on fluid dynamics.)
- (please refer to guidance produced by US NiH, US CDC, University of Minnesota Center for Infection Disease Research and Policy on rates of sufficient ventilation; see, for a start, Kumar and Morawska, City and Environment Interactions, 2019; Li, et al, ‘Evidence for probable aerosol transmission of SARS-Co-V-2 in a poorly ventilated restaurant’, 2020. For lay science, there are some very good recent articles in The Conversation on fluid dynamics.)
- How will rooms be cleaned after use?
- How much time will rooms be empty (airing) after one session before another session can enter?
- What kind of signage will be placed on doors indicating that rooms are not to be entered (e.g. Room being aired – do not enter). Please reference risk assessments that note rooms must remain vacant for set periods after use.
- What are the mechanisms for reporting at-work contracting of Covid-19 to HSE? How often will this take place?
- How is travel to campus via public transport being risk assessed for staff return to on-campus work?
- How will first aiders respond? How will they be protected?
- Will Keele be providing all required PPE for staff and students, including disposable face masks?
- What is Keele doing to ensure that people do not have to choose between their jobs and the safety of their family? Please ask management to remember that Keele is full of very intelligent people who are able to read the evidence, so they would benefit from not assuming otherwise in their answers to any questions.
- Who is doing the risk assessments? Who is saying what needs to be done in order to be safe? If not a scientific or medical specialist, how are they qualified to do this for a highly contagious virus that can severely affect anyone, regardless of whether or not they have a health condition?
- Are risk assessments for teaching buildings/spaces considering capacity limits for rooms, for corridors, social spaces, toilets, kitchens, photocopy rooms, and transit routes? This must include assessment of accessible routes for disabled users.
- Are risk assessments and determining what is safe informing re-opening plans, or are re-opening plans determining what risk assessments say? I would not be surprised if it was the latter.
- Multi-use buildings must have processes and physical barriers that clearly separate social/catering from academic use. Movement around buildings must accommodate for this separation. How is this going to happen in buildings like Chancellor’s, David Weatherall, KMS, and the Library, for example?
- In terms of ongoing identification of hazards, what are the routes for immediate action on problems/imminent harm?
- Who is responsible for writing safe systems of work (likely to be multiple per activity/space)? When will these be completed?
- Who is responsible for implementing controls and mitigations? Who is responsible for monitoring and ensuring compliance? For large buildings where there certainly have to be multiple points of control, how are they ensuring that all points are coordinated and working together consistently and regularly?
- Are all of the people doing risk assessments experienced enough in the spread of viral pathogens? If not, what ‘competent person’ is assisting them? I know many of my colleagues have been working on risk assessments, but I also know they are experienced and have no doubt of their competence. Is this the same for all parts of the university?
- Who is responsible for appropriate training of staff and students (please note: this must be an appropriate training activity that is properly designed and taught by trained individuals. It must be mandatory, CANNOT be online – too easy to cheat the system. We all know this because we all do it).
- Who is responsible for producing clear instructions documentation for staff?
- What I the escalation route for staff if there are concerns in their area?
- What is the health surveillance system/processes at Keele, and how are these linked to local systems/processes? (local here: not just Newcastle/Stoke, but local area to include commutable areas (Crewe, Derby, Manchester, Stafford, Shrewsbury, Birmingham, etc.)).
- In terms of competency requirement in risk assessments – who has virology and epidemiology competency in the risk assessment team? If no one, what competent individual/s are being consulted throughout the risk assessment process? (please say they’re not working only off of general guidance. That’s not how you keep staff and students safe).
- Who do I sue when I get Covid from work because I’ve been forced into an unsafe work environment when I could have done that work remotely? (Anyone who has been following the evidence lately can see that sitting in an indoor teaching space where people are talking for an hour is going to be unsafe, regardless of how many times we wash our hands.)